Plant Sterols for Cholesterol: The Evidence, the Dose, and What to Expect
Plant sterols are one of the few cholesterol-lowering supplements that major cardiovascular guidelines actually acknowledge. Not as a replacement for medication in high-risk patients — the guidelines are clear on that — but as a legitimate, evidence-supported dietary adjunct for people with mild-to-moderate LDL elevation managing through lifestyle.
Most online information either overpromises or dismisses them entirely. What the evidence shows is more specific: plant sterols work — but only at the right dose, only taken correctly, and only in the right context.
What plant sterols are and how they work
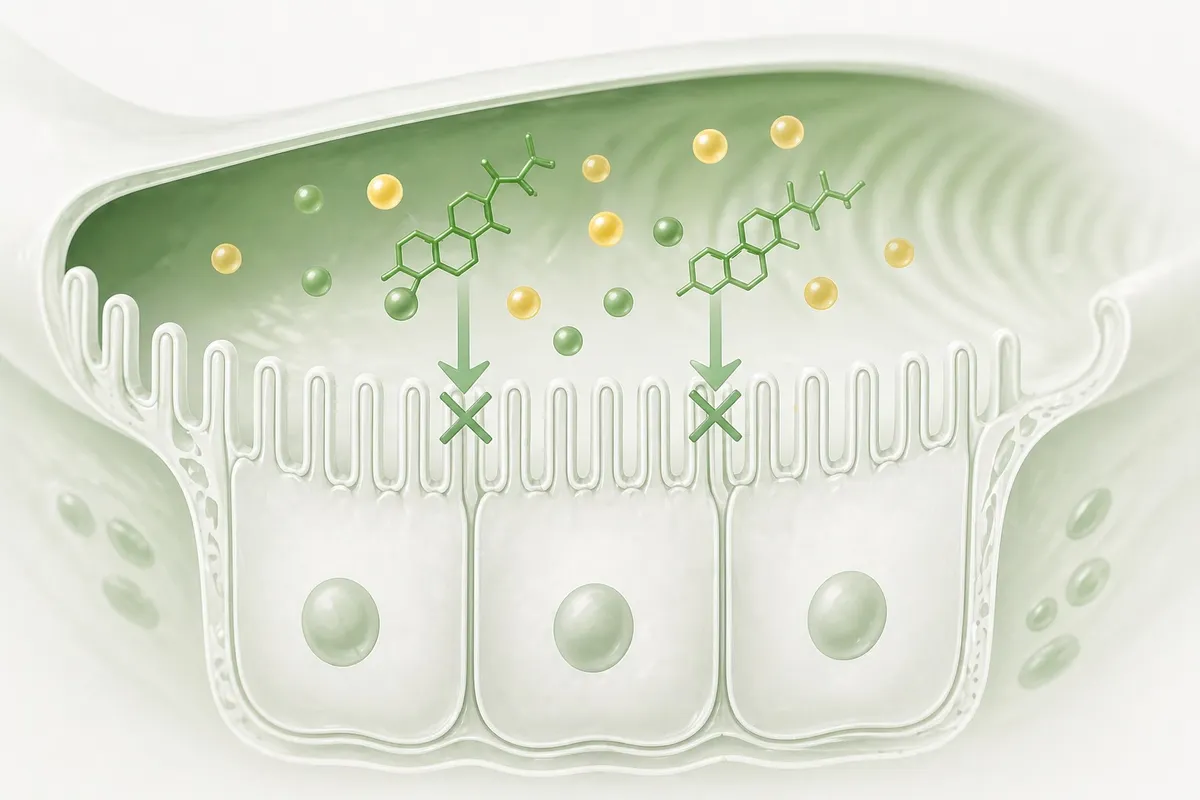
Plant sterols (also called phytosterols) are naturally occurring compounds found in plant cell membranes. Structurally, they closely resemble cholesterol — which is exactly why they work.
When you eat plant sterols, they compete with dietary cholesterol for absorption in the small intestine. They occupy the same absorption sites — effectively blocking some dietary cholesterol from entering the bloodstream. The liver compensates by pulling more LDL from the blood, which is why the LDL-lowering effect occurs.
What the evidence shows
The core finding
A 2014 meta-analysis published in the British Journal of Nutrition, analyzing 124 randomized controlled trials, found that plant sterols at approximately 2g/day reduced LDL cholesterol by a mean of 8.3% compared to placebo. The effect was consistent across populations, food formats, and study durations.
The dose-response relationship
| Daily dose | Approximate LDL reduction |
|---|---|
| 0.5g | ~3% |
| 1.0g | ~5% |
| 1.5g | ~7% |
| 2.0g | ~8–10% |
| 3.0g+ | ~10–11% (diminishing returns) |
Additive with statins and the Portfolio Diet
Plant sterols work through a different mechanism than statins — absorption vs. production. Their effects are additive. A meta-analysis in JACC found that adding plant sterols to statin therapy produced an additional LDL reduction of approximately 10% on top of whatever the statin was already achieving.
Regulatory recognition
The FDA has an authorized health claim: foods containing at least 0.65g of plant sterol esters per serving (total 1.3g/day) with meals as part of a diet low in saturated fat may reduce the risk of heart disease. EFSA has authorized a parallel health claim in Europe. The European Atherosclerosis Society consensus statement explicitly lists plant sterols as a non-prescription LDL-lowering option with an expected 8–10% reduction at 2g/day.
How to use plant sterols correctly
Dose: 2g per day
Check labels carefully — “plant sterols” and “plant stanol esters” are measured differently. Look for the amount of sterol or stanol content, not the total weight of the product.
Timing: with meals — this is not optional
Duration: 6–8 weeks to see results
LDL reduction from plant sterols is not immediate. The effect becomes measurable after approximately 6–8 weeks of consistent daily use. Plan to retest your lipid panel after 8–12 weeks.
One contraindication to know
What plant sterols don’t do
They don’t lower triglycerides. For elevated triglycerides, dietary carbohydrate reduction and omega-3 fatty acids are more relevant.
They don’t raise HDL. For HDL, exercise and smoking cessation are the most effective lifestyle interventions.
The effect stops when you stop. LDL returns to baseline within weeks of stopping. This is a daily habit, not a short course.
Combining plant sterols with the Portfolio Diet
| Intervention | LDL reduction |
|---|---|
| Plant sterols 2g/day with meals | 8–10% |
| Psyllium fiber 10g/day | 5–7% |
| Soy protein 25g/day | 3–5% |
| Nuts 30g/day | 3–5% |
| Replacing saturated fat with PUFA | 5–8% |
| Combined (real-world adherence) | 15–25% |
Find out if plant sterols are right for your situation
The right intervention depends on where you actually sit on the risk spectrum. Our quiz analyzes your full profile in 2 minutes.
Take the 2-minute quiz → Free · No account required · Based on 2026 clinical guidelinesSources
- Ras RT, et al. LDL-cholesterol-lowering effect of plant sterols and stanols across different dose ranges. Br J Nutr. 2014;112(2):214-219. PMID: 24780090
- Gylling H, et al. Plant sterols and plant stanols in the management of dyslipidaemia (EAS Consensus). Atherosclerosis. 2014;232(2):346-360. PMID: 24468148
- EFSA Panel on Dietetic Products. Scientific Opinion on health claims related to plant sterols. EFSA Journal. 2012;10(5):2692.
- Scholle JM, et al. The effect of adding plant sterols or stanols to statin therapy. J Am Coll Cardiol. 2009. PMID: 19576352
- Demonty I, et al. Continuous dose-response relationship of the LDL-lowering effect of phytosterol intake. J Nutr. 2009;139(2):271-284. PMID: 19091798
- Berge KE, et al. Accumulation of dietary cholesterol in sitosterolemia. Science. 2000;290(5497):1771-1775. PMID: 11099417